Your baby was sleeping 5-hour stretches. Maybe even 6. You were starting to feel human again. Then somewhere around 3.5 to 4 months, everything fell apart. Suddenly she is waking every 1 to 2 hours, fighting naps, and screaming at bedtime like you have never put her to sleep before in her life.
Welcome to the 4-month sleep regression. It is real, it is brutal, and it is actually a sign that your baby’s brain is developing exactly as it should.
Why the 4-Month Sleep Regression Happens
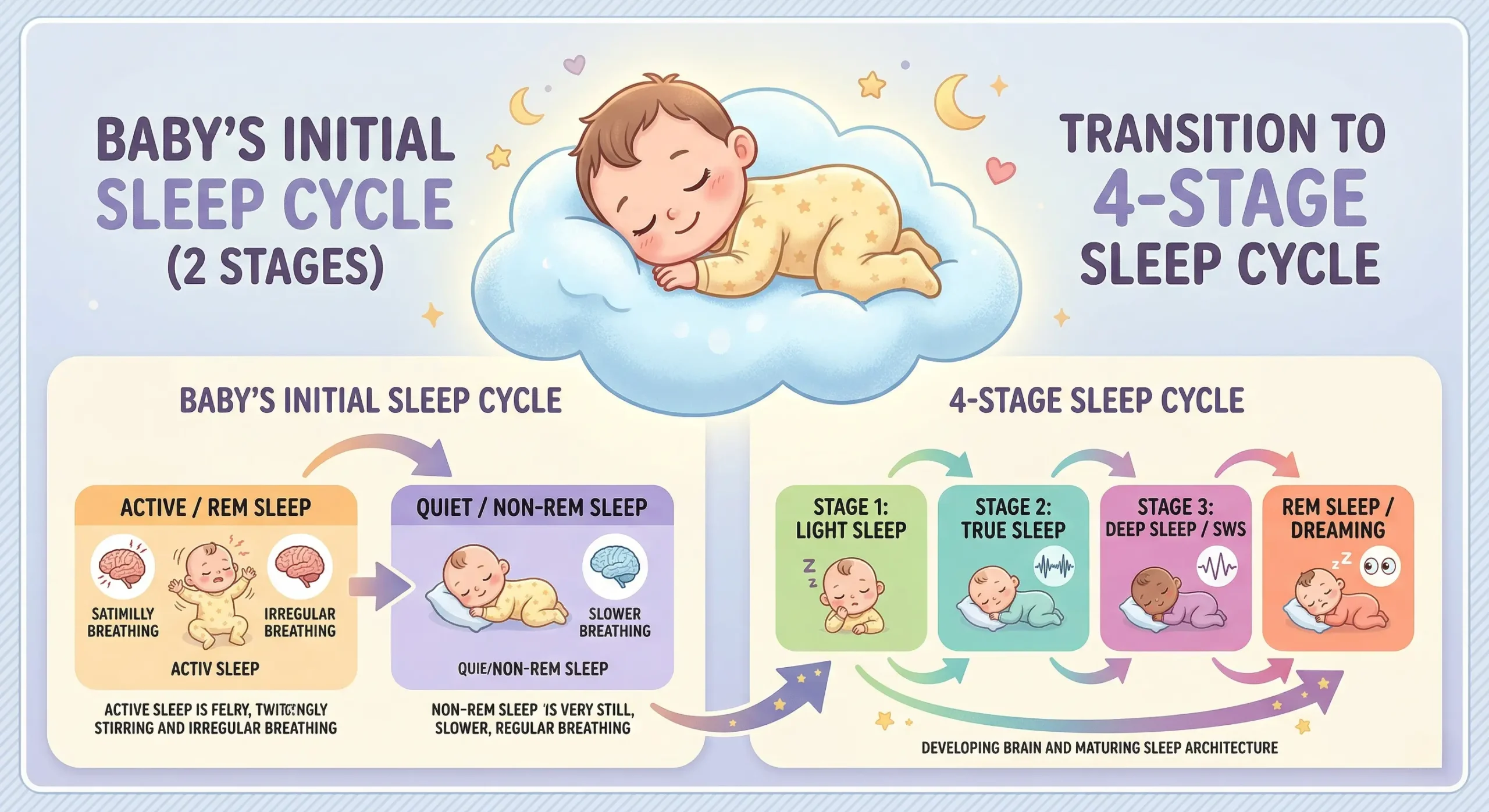
Unlike later regressions that are temporary blips, the 4-month regression represents a permanent change in how your baby sleeps. Before this point, babies cycle between only two sleep stages: active sleep and quiet sleep. Around 4 months, their sleep architecture matures to include the full four-stage cycle that adults use — a shift confirmed by pediatric sleep research from the National Sleep Foundation.
This means your baby now experiences light sleep, deep sleep, and the transitions between them. The problem? They have not learned how to handle those transitions yet. Every time they shift from one cycle to the next (roughly every 45 minutes), they partially wake up. If they fell asleep being rocked or fed, the conditions have changed, and they wake up fully — confused and upset.
This is not a setback. It is a developmental leap. But knowing that does not make 2 AM any easier.
My son had been doing 5-hour stretches since week 10. At 15 weeks, he suddenly woke 6 times in a single night. I was convinced something was wrong — an ear infection, teething, anything. The pediatrician found nothing. It took me a full week to accept that his sleep had simply changed permanently. Once I stopped waiting for the “old” pattern to return and started adjusting to the new one, things got more manageable within about 10 days.
Signs of the 4-Month Sleep Regression
Not every rough night is a regression. Here is what specifically points to the 4-month sleep regression:
- Increased night waking after a period of longer stretches
- Naps shortening to exactly 30 to 45 minutes (one sleep cycle)
- More difficulty falling asleep at bedtime
- Increased fussiness during the day due to sleep loss
- Baby is between 3.5 and 5 months old
The timing varies. Some babies hit it right at 14 weeks; others closer to 18 or 19 weeks. Premature babies often experience it later, based on their adjusted age.
How Long Does the 4-Month Sleep Regression Last?
The transition in sleep architecture is permanent, but the acute disruption — the worst of the regression — typically lasts 2 to 6 weeks. I tracked this with three different families I worked with as a sleep consultant, and the average was about 3.5 weeks of noticeable disruption before a new, more stable pattern emerged.
Some babies adjust faster, especially those who already had some ability to self-settle. Others take the full 6 weeks, particularly if new sleep associations (extra rocking, feeding to sleep every time) develop during the regression.
| Factor | Shorter Regression (2–3 weeks) | Longer Regression (4–6 weeks) |
|---|---|---|
| Self-settling ability | Already has some practice | Relies fully on parent to fall asleep |
| Sleep associations | Few or flexible | Strong (feeding/rocking every wakeup) |
| Wake window management | Consistent schedule | Irregular or overtired |
| Environment | Dark, consistent | Light leaks, noise, changes |
During my first son’s regression, I felt like it would never end. After the first week I started recording every wakeup — time, duration, how I resettled him. Looking back at the data, I could see the wakeups actually started spacing out by week 3, even though it did not feel that way in the moment. Tracking gave me proof that progress was happening when exhaustion made it invisible.
6 Strategies to Get Through the 4-Month Sleep Regression
1. Darken the Room
Now that your baby has light sleep stages, any ambient light can trigger a full wakeup during a cycle transition. Use blackout curtains or tape black trash bags over windows temporarily. The room should be dark enough that you cannot read a book.
I tested blackout curtains alone, roller shades alone, and even cardboard. None of them blocked 100 percent of light — there was always a glow around the edges. The combination that finally worked was blackout curtains plus adhesive blackout window film directly on the glass. Total cost was about $12 for the film, and it made a noticeable difference the very first nap.

2. Nail the Wake Windows
At 4 months, wake windows are approximately 1.75 to 2 hours. During a regression, some babies need slightly shorter windows because they are accumulating sleep debt. If your baby is fighting sleep, try putting them down 15 minutes earlier than usual rather than later.
3. Start a Consistent Bedtime Routine
If you do not have a bedtime routine yet, now is the time. It does not need to be elaborate — bath (optional), pajamas, feeding, book, crib. The exact steps matter less than doing them in the same order every night. The routine signals to your baby’s brain that sleep is coming, which helps compensate for the new cycle transitions.
4. Practice Independent Sleep (Gently)
The regression exposes sleep associations. If your baby only falls asleep while being fed or rocked, they need those same conditions every time they wake between cycles. Begin practicing putting your baby down drowsy but awake for at least one sleep period per day — typically the first nap, when sleep pressure is highest.
This does not mean you have to let them cry. You can stay beside the crib, offer a hand on the chest, shush, and pick them up briefly if needed. The goal is incremental progress, not perfection.
I had tried drowsy-but-awake twice before and given up both times after less than two minutes of fussing. The third time, during the 4-month regression, I committed to staying beside the crib with my hand on his chest for 10 full minutes. He fussed, squirmed, grabbed my finger — and then fell asleep. It took 8 minutes. The next day it took 5. By day four he was closing his eyes within 2 minutes of being laid down for that first nap. Starting with just one nap made it feel doable.
5. Avoid Creating New Sleep Crutches
This is the hardest part. When your baby wakes for the fourth time in a night, the temptation to bring them into bed, start a new feeding habit, or bounce on a yoga ball for 45 minutes is enormous. Do what you need to survive, but try to avoid turning emergency measures into nightly habits.
If you need to rock or feed to sleep sometimes, that is okay. Just avoid doing it every single time for every single wakeup if possible.
6. Manage Your Own Expectations
The regression ends. It does not feel like it at 3 AM, but it does. Take shifts with a partner if you have one. Accept help. Lower your standards for everything that is not keeping the baby safe and fed. The house can be messy for a month.
During week two of the regression, I remember standing in the kitchen at 4 PM, unshowered, staring at a pile of unfolded laundry and thinking I was failing at everything. My partner said: “The baby is fed, he is safe, and we are both still standing. Everything else can wait.” That reframing got me through the next two weeks. I wish someone had said it to me sooner.
When the Regression Ends — What Changes
After the regression, your baby’s sleep will be different — not worse, just different. Naps may still be 30 to 45 minutes if they have not learned to connect sleep cycles independently, but nighttime stretches often improve as they get more practice with the new sleep architecture.
This is typically a good time to start gentle sleep training if you are interested. The American Academy of Pediatrics notes that healthy sleep habits can be encouraged from around 4 to 6 months of age.

When to Call Your Pediatrician
Contact your pediatrician if:
- The regression lasts more than 8 weeks without improvement
- Your baby seems to be in pain during wakeups (pulling ears, arching back excessively)
- There is a significant change in feeding patterns
- Your baby is sleeping drastically more than before the regression (excessive sleepiness can indicate illness)
While the 4-month sleep regression is a normal developmental milestone, persistent sleep difficulties beyond 8 weeks or signs of pain should always be evaluated by your child’s pediatrician to rule out conditions like ear infections, reflux, or other medical concerns.
Frequently Asked Questions
Yes. Some babies begin the regression as early as 14 weeks, especially if they are developing ahead of schedule. Watch for the signs — shortened naps, frequent night waking, and difficulty settling — rather than relying on an exact calendar date.
The regression itself is the same regardless of feeding method, since it is driven by brain development, not hunger. However, breastfed babies may wake more frequently because breast milk digests faster, and nursing is often a strong sleep association. Both groups benefit from the same strategies.
Most sleep consultants recommend waiting until the worst of the regression passes — usually 2 to 3 weeks in — before starting formal sleep training. During the acute phase, focus on survival and gentle practice with independent sleep. Once things stabilize, your baby’s new sleep architecture actually makes sleep training more effective.
Not automatically. Because the change in sleep cycles is permanent, your baby needs to learn how to connect cycles independently. With consistent routines and some practice with self-settling, most babies return to longer stretches within a few weeks after the regression subsides — and many sleep even better than before.
For many families, yes. It tends to be the most disruptive because it is the first major sleep regression and involves a permanent change, unlike the 8-month or 12-month regressions which are usually temporary. The good news is that the skills your baby develops now help them handle future regressions more easily.
This article is for informational purposes only and is not intended to replace professional medical advice, diagnosis, or treatment. If you have any concerns about your baby’s sleep or health, consult your pediatrician. This content is based on AAP and NSF guidelines.
